Pizza or Pasta tonight? Why not!
Dietitian & Nutritionist in Brussels · NIHDI-Registered
Nothing Forbidden.Eat With PleasureAchieve Your Goals
Monash FODMAP Certified
Your Nutrition Partner
Maybe hunger has been your shadow through every diet. Maybe FODMAP promised clarity but gave you questions. Maybe you quit when healthy eating became joyless – and here's the truth: you weren't asking too much. You were given too little.
No Restrictions
Eat What You Love

8 Gateways Across Brussels
Your Transformation Starts Here
Every office is a starting point to a healthier life. Find the one that's right for you.
Video Consultation
From home, anywhere in Belgium
Latest Insights
Evidence-Based Nutrition Guidance
Discover the latest research, practical tips, and evidence-based strategies to improve your health.

IBS & FODMAP
38 min read
Irritable Bowel Syndrome: Rome V Criteria and Treatment in 2026
The Rome V consensus, published in early 2026, redefines irritable bowel syndrome. Discover what changes in diagnosis, what research reveals about its autoimmune mechanisms, and how current treatments combined with personalised nutrition restore your digestive comfort.
Pierre Abou-Zeid
Read article

gut-health
42 min read
The SIMO, SIBO and IMO Spectrum: Pathophysiology, Diagnosis and Treatment
Microbial imbalance in the small intestine is not limited to bacteria. Discover the SIMO spectrum, its four forms (SIBO, IMO, hydrogen sulphide, SIFO), how each is diagnosed and treated, and how phased personalised nutrition restores your digestive comfort without deprivation.
Pierre Abou-Zeid
Read article
gut-health
45 min read
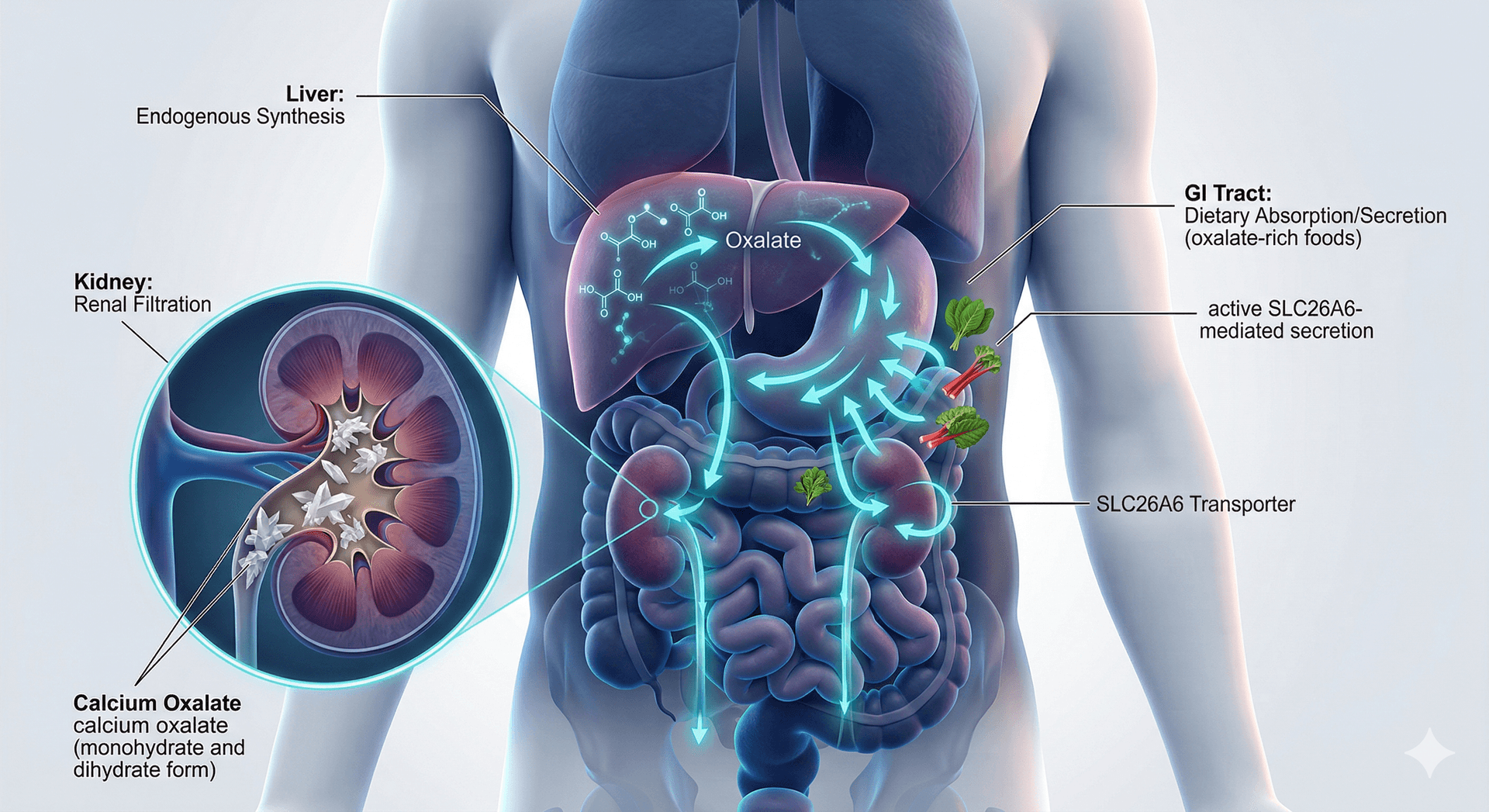
Comprehensive Analysis of Oxalate Metabolism, Intestinal Transport Mechanisms, and Dietary Therapeutics
Oxalate cannot be degraded by human cells — its systemic control depends entirely on renal and intestinal excretion. This advanced review covers hepatic synthesis pathways, SLC26A6/SLC26A3 transport kinetics, tight-junction permeability, microbiome-mediated degradation, and a complete clinical food database for dietary therapeutic guidance.
Pierre Abou-Zeid
Read article